
Balwant Singh Bains
Department of Physiotherapy, Aihmsa College,
Kuala Lumpur, Malaysia
Fahimeh Khoshmaram
Department of Sports Biomechanics,
Faculty of Physical Education and Sports
Sciences, Kharazmi University, Tehran, Iran
Mandeep Singh Bains (Corresponding author)
R&D Division, BainsPhysio,
9127, Jalan Bandar 4, Taman Melawati,
53100 Kuala Lumpur, Selangor, Malaysia
Received: 01-10- 2018
Published: 01-01- 2019
Abstract
Background: A condition of the knee bending forward too far beyond the locking position is called hyperextended knee. It occurred primarily as a birth defect but can be augmented with high-impact events, and these predisposing factors in athletes bring about risk to the lower limb. Although this injury is painful, it is easy to treat if it is spotted sooner especially picked up during Joints’ Functional screening.
Objective: The objective of this study was to investigate the prevalence of hyperextended knee among older adults.
Method: Four hundred healthy volunteers between the ages of 40 to 60 years participated in this study. In order to measure severity of knee hyper-extension among participants, plinth measurement scale (self-created) was used.
Results: Approximately 38% of participants had patchy flexibility limitation and 90% of the 38% had knee hyperextension issues.
Conclusion: This study revealed the prevalence of knee joint hyperextension in older adults and as population is aging all over the world, treatment of this malposition of the knee in older adults should be considered as a priority.
Keywords: Knee joint, Hyperextended Knee, Joint hypermobility Adult, range of motion
1. Introduction
Hyperextended (Genu Recurvatum) knee means extension of the knee beyond the neutral anatomical position (Cooper, Alghamdi, Alghamdi, Altowaijri, & Richardson, 2012).Knees hyperextended is the common problem among children and adults. Weight bearing with knees hyperextended, together with reduced motion control arising from poor proprioceptive acuity, and reduced muscle strength and endurance to control this movement, may cause repetitive micro-trauma and abnormal loading of the knee joint, resulting in knee pain (Pacey, Tofts, Adams, Munns, & Nicholson, 2013). In addition, genurecurvatum may experience knee pain, display an extension gait pattern and poor proprioceptive control of terminal knee extension (de Sá Pinto, de Barros Holanda, Radu, Villares, & Lima, 2006). Knee hyperextended problem leads to injuries and increase risk of fall among elderly people. The posterior cruciate ligament (PCL) and
anterior cruciate ligament (ACL) act as main ligaments and are frequency injured. The consequences of knee injuries with extrinsic and intrinsic risk factors are significant causes of concern for the physiotherapist (Bahr & Holme, 2003). Loading of stress takes place at the patellar tendons and the anterior structures of knee joints. Weakness of lower limb muscles, specially gastrocnemius, and hamstring , is recommended as a possible cause of hyperextended knee (Moseley, Wales, Herbert, Schurr, & Moore, 1993). Cooper (2005) found that hamstring muscle weakness was the reason of knee hyperextension in some participants and in some others, quadriceps muscle was weak(Cooper, 2005). On the other hand, study of Bleyenheuft, Hanson, & Deltombe (2010), mentioned that weakness and spasticity of the knee extensors and weakness of knee flexors (the hamstring muscles) are the causes of genu recurvatum. Strengthening exercises for hyperextended knee can help to return knee to original level of stability. Some studies reported that knee hyperextended may lead to abnormal gait, unbalance and increase risk of fall among older adults(Noyes, Dunworth, Andriacchi,
Andrews, & Hewett, 1996). in addition knee hyperextend may be the initial reason of knee osteoarthritis among older adults (D’Gasper, Bains, Sadeghi, & Kumar, 2018). To overcome the mentioned problems, finding the rate of hyperextended knee among older adults is necessary. The objective of this study was to reveal the prevalence of knee hyperextension among individuals over 40 year old. The method used to justify this, JFS (Joint’s Functional Screening) system was introduced to early detect the condition in normal individuals at the age of 40 (Bains, 2018).
2. Method
Study Design and Participants
This study was a cross-sectional survey to investigate the prevalence of hyperextended knee among older adults. Four hundred healthy volunteers in ages of 40 to 60 years (49±5.2), participated in this study. Participants were selected from the clients in BainsPhysio® (A Physiotherapy Clinic) at Taman Melawati, Kuala Lumpur, Malaysia where the public in the surrounding community came for Joint Functional Screening (JFS) and other conditions needing physiotherapy. All participants signed a consent form before starting the study and were screened for eligibility by the senior physiotherapists.
Test Procedure
In order to measure severity of knee hyper-extension among participants, plinth measurement scale (self-created) was used. Less than 1 inch from plinth was considered as 1st Degree; more than 1 inch but less than 2 was considered 2nd degree and more than 2 inches but less than 3 inches was taken as 3rd. degree. Anything more than 3 inches were taken as 4th degree. Measurements were by ruler from the apex of the heel to the plinth level in the supine position.
Statistical analysis
Descriptive statistical analyses of the data were executed by SPSS software version 22. The frequencies, percentages, and graphical analysis of the data were displayed.
3. Results
| Variables | Mean and SD |
| Age | 52.01±2.34 |
| BMI | 24.85±2.88 |
Table 1: Characteristics of Participants
From the JFS analysis among city dwellers, 38% of participants had patchy flexibility limitation and 90% of the 38% people had knee hyperextension issues. The following chart shows the percentage of them with varying degree of hyper extension. As mentioned, above 90% of the participants had hyper-extension of knee joints either on one or both knees.
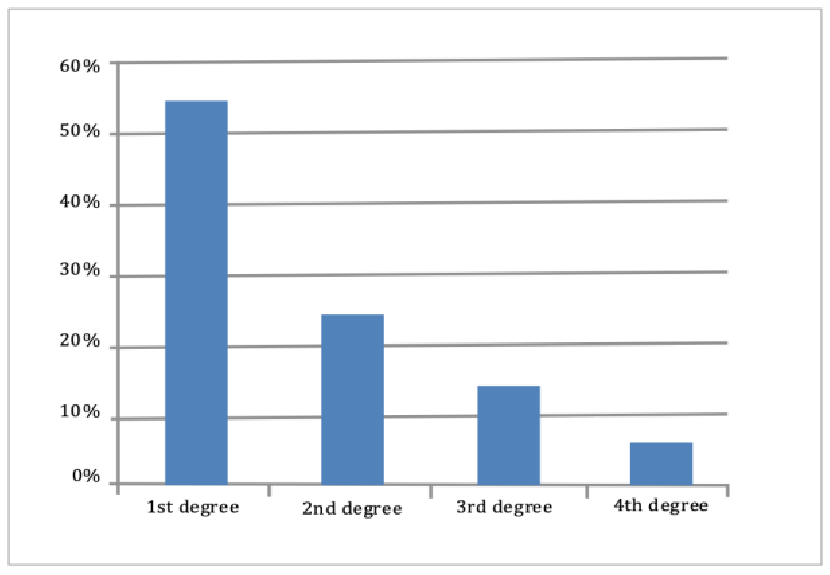
Figure 1: Rate of knee hyperextension among adults
The results of survey showed that Among those with hyper-extension of knee, 55 % had 1st degree , 25 % had 2nd degree , 15 % had 3rd. degree , and 5% had 4th degree hyper- extension.
4. Discussion
The evaluation of 400 older adults referred to a Physiotherapy Clinic for musculoskeletal problems showed that 38% of the study group had hyper extension of knee. Patients with joint hypermobility usually presents back pain, arthralgia, recurrent joint dislocation or subluxation, if they are in the category 4th degree or osteoarthritis (Seçkin et al., 2005).
Although a direct association between joint hypermobility, joint or soft tissue injury, and osteoarthritis cannot be made from this study, in previous literature, laxity of the joints has been introduced as a predisposing factor for joint or soft tissue injury(Biro, Gewanter, & Baum, 1983). It can also be a hypothetical conclusion that one of the causes of hyper extended knee could be early walking in childhood where walkers are introduced before walking milestone in babies.
The pathogenesis of osteoarthritis may be related to abnormal joint biomechanics of stress. On the other hand, the abnormal ‘loose’ connective tissue in hypermobile joints leads to abnormal joint biomechanics(Grahame, 1989). Thus, it could be concluded that hypermobility of joints may lead to osteoarthritis.
One study conducted by Noyes et al. (1996) investigated gait abnormalities in unstable knees and concluded that using gait analysis techniques, patients with severe ligamentous injuries can alter the biomechanics of hip, knee, and ankle function to more normal levels(Noyes et al., 1996). They stated that appropriate gait adaptations resulting from careful instruction and extensive physiotherapy aided exercise have a place in the treatment of knees with complex ligament
injuries.
The exact cause of hyperextended knee is unclear, but the hereditary nature of hypermobility is suggested by some studies(Seçkin et al., 2005). Also, the previous studies demonstrated that hypermobility is more common in younger (Grahame, 1990) but this study revealed the prevalence of this abnormality among older adults which should be investigated more in future studies. As population is aging in most parts of the world (Anderson & Hussey, 2000), paying attention to the physicals problems of adults and suggesting solutions to overcome the problems seem to be necessary. As we have found joint hypermobility was common in 90% of the group mentioned. It should be also noted that the prevalence of gastrocnemius junction and patellar tendon, depends on the degree of hyperextension in subjects without any symptoms of pain. This needs early treatment by physiotherapy means. It is important for doctors & health service providers to recognise this problem to ensure correct diagnosis and treatment and early referral to physiotherapist for tailor-made exercise. Joint hypermobility may cause severe functional problems for adults.
5. Conclusion
This study revealed the prevalence of knee joint hyperextension in older adults which is a malposition between the femur and tibia and causes many functional problems and diseases. As population is aging, Treatment of this postural fault in older adults should be considered a priority. Further evaluation of the association between joint hypermobility and diseases is needed.
References
Anderson, G. F., & Hussey, P. S. (2000). Population aging: a comparison
among industrialized countries. Health affairs, 19(3), 191-203.
Bahr, R., & Holme, I. (2003). Risk factors for sports injuries—a methodological approach. British Journal of Sports Medicine, 37(5), 384-392.
Bains, B. S. (2018). Joint Functional Screening (JFS): Movement for
Optimal Health and Body Function: Perspective Clinical Examination.
Rehabilitation Science, 3(1), 13.
Biro, F., Gewanter, H. L., & Baum, J. (1983). The hypermobility syndrome.
Pediatrics, 72(5), 701-706.
Bleyenheuft, C., Bleyenheuft, Y., Hanson, P., & Deltombe, T. (2010). Treatment of genu recurvatum in hemiparetic adult patients: a systematic literature review. Annals of physical and rehabilitation medicine, 53(3), 189-
199.
Cooper, A. (2005). Relationship of hemiparetic gait patterns to
underlying neurological impairment and its relevance to physiotherapeutic
intervention. Cardiff University.
Cooper, A., Alghamdi, G. A., Alghamdi, M. A., Altowaijri, A., & Richardson, S.
(2012). The relationship of lower limb muscle strength and knee joint
hyperextension during the stance phase of gait in hemiparetic stroke
patients. Physiotherapy research international, 17(3), 150-156.
D’Gasper, D., Bains, B., Sadeghi, H., & Kumar, P. (2018). Comparing Exercise Prescription Methods in Knee Osteoarthritis Patients in Malaysia. Acta Medica Bulgarica, 45(1), 26-31.
Grahame, R. (1989). How often, when and how does joint hypermobility lead to osteoarthritis? British journal of rheumatology, 28(4), 320.
de Sá Pinto, A. L., de Barros Holanda, P. M., Radu, A. S., Villares, S. M., & Lima, F. R. (2006). Musculoskeletal findings in obese children. Journal of
paediatrics and child health, 42(6), 341-344.
Grahame, R. (1990). ‘The hypermobilitysyndrome’. Annals of the rheumaticdiseases, 49(3), 199.
Moseley, A., Wales, A., Herbert, R., Schurr,K., & Moore, S. (1993). Observationand analysis of hemiplegic gait: stancephase. Australian journal ofphysiotherapy, 39(4), 259-267.
Noyes, F. R., Dunworth, L. A., Andriacchi, T.P., Andrews, M., & Hewett, T. E.(1996). Knee Hyperextension GaltAbnormalities in Unstable Knees: Recognition and Preoperative GaitRetraining. The American journal ofsports medicine, 24(1), 35-45.
Pacey, V., Tofts, L., Adams, R. D., Munns, C.F., & Nicholson, L. L. (2013).Exercise in children with jointhypermobility syndrome and kneepain: a randomised controlled trialcomparing exercise into hypermobileversus neutral knee extension. Pediatric Rheumatology, 11(1), 30.
Seçkin, Ü., Tur, B. S., Yılmaz, Ö., Yağcı, İ.,Bodur, H., & Arasıl, T. (2005). Theprevalence of joint hypermobilityamong high school students. Rheumatology international, 25(4),260-263.
